
What's the Sniff with C. diff?
Clostridioides difficile, or more commonly referred to as "C. diff," is a toxin-producing, spore-forming gram-positive anaerobic bacilli. C. diff infections are a growing concern for health care systems in 2022.


Author: Ashley Wensing, PharmD
Editor: Kristen Lindauer, PharmD
This week's article is brought to you from an in-service presentation created by Ashley Wensing, a current PGY1 Pharmacy Resident at OSF Saint Francis Medical Center. Dr. Wensing presented on the topic "IDSA-SHEA Clostridioides difficile Infection (CDI) in Adults - 2021 Updates" during one of her APPE rotations as a fourth-year pharmacy student in January of 2022.
A recent initiative in health systems has been reducing the rates of Clostridioides difficile testing, infection, and recurrence. Today, we will cover the basics of testing, preventing the spread of disease, and dive into the updates on treatment for CDI.
Special edition: At the bottom of this article are two patient cases to test your knowledge. Enjoy!
Disclaimer: This post is meant to provide an overview of a clinical topic that may include (but is not limited to) information on pathophysiology, diagnosis, treatment, clinical pharmacology, medication management, adverse effects, and clinical pearls. References are included at the bottom of each post. This post is not to be used as medical advice for direct patient care, but as a guide for learning and discussion.
Background
Clostridioides difficile, or more commonly referred to as "C. diff," is a toxin-producing, spore-forming gram-positive anaerobic bacilli.
Toxins A and B
- Toxin B is much more potent, a cytotoxin for most cell lines, and recent data suggests that toxin B can cause disease alone.
- A-B+ are found worldwide and are responsible for well-documented diseases. Also, these are associated with severe intestinal and systemic organ damage and induce inflammatory responses.
- In contrast, A+B- has no compelling evidence to exist naturally.
Transmission of C. diff is facilitated by spores. The spores can spread by person-to-person through the fecal-oral route or through exposure to contaminated surfaces or equipment. Spores can survive on dry inanimate surfaces for up to 5 months! To reduce transmission, especially in the hospital setting, it is recommended to wash your hands with soap and water, NOT with alcohol-based hand sanitizer.

Clinical Presentation/Diagnosis
Preferred target population to test: patients with 3 or more unexplained and new-onset unformed stools in 24 hours.

Diagnosis is done by a stool toxin test:
- Glutamate dehydrogenase (GDH) + toxin; or
- GDH toxin, arbitrated by nucleic acid amplification test (NAAT); or
- NAAT + toxin
Treatment

There are 3 major updates from 2017 --> 2021 IDSA-SHEA guidelines:
Update/question #1: In patients with an initial CDI episode, should fidaxomicin be used rather than oral vancomycin?
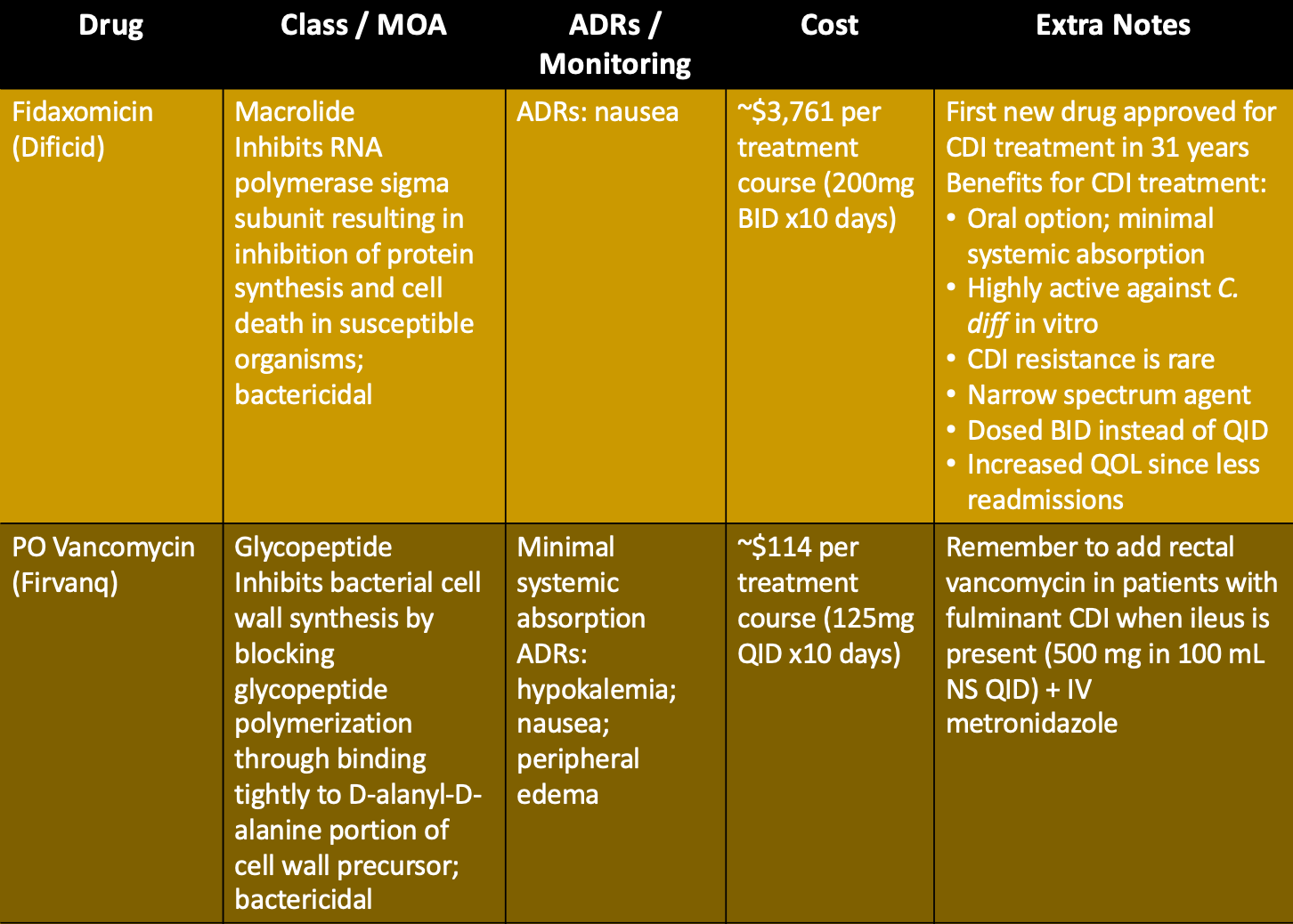
- Answer: Yes, updated 2021 IDSA-SHEA guidelines recommend using fidaxomicin rather than a standard course of oral vancomycin. However, oral vancomycin remains an acceptable alternative.
- Evidence: 4 RCTs - 2 mentioned in 2017 guidelines and 2 recently published trials.
Update/question #2: In patients with recurrent CDI episode(s), should fidaxomicin be used rather than oral vancomycin?
- Answer: Yes, updated guidelines recommend fidaxomicin rather than a standard course of oral vancomycin. However, oral vancomycin pulsed or as a standard regimen is an acceptable alternative.
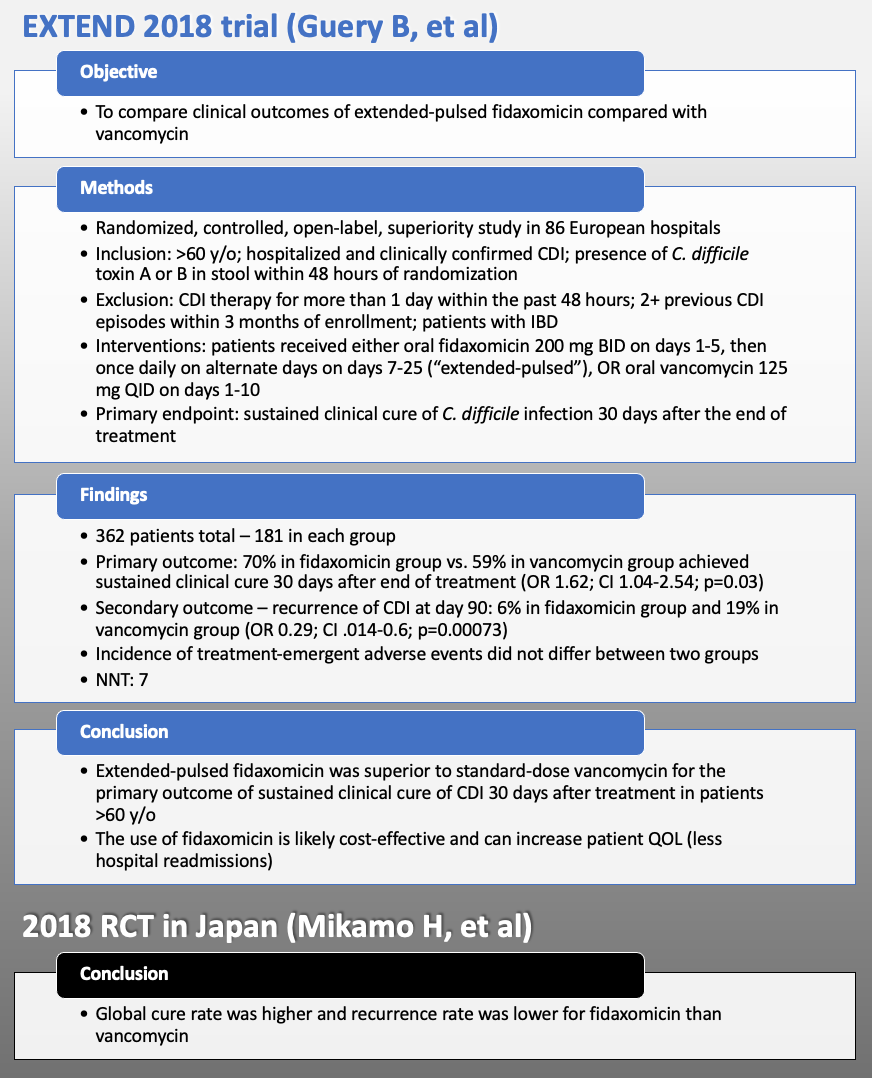
- Evidence: Subgroup analysis of 3 RCTs – 2 mentioned in 2017 guidelines, as well as the EXTEND trial. Pooled analysis shows that fidaxomicin increased sustained response of CDI 30 days after end of therapy compared with vancomycin (RR 1.27; CI 1.05-1.54) in patients experiencing recurrent CDI (≥1 recurrence).
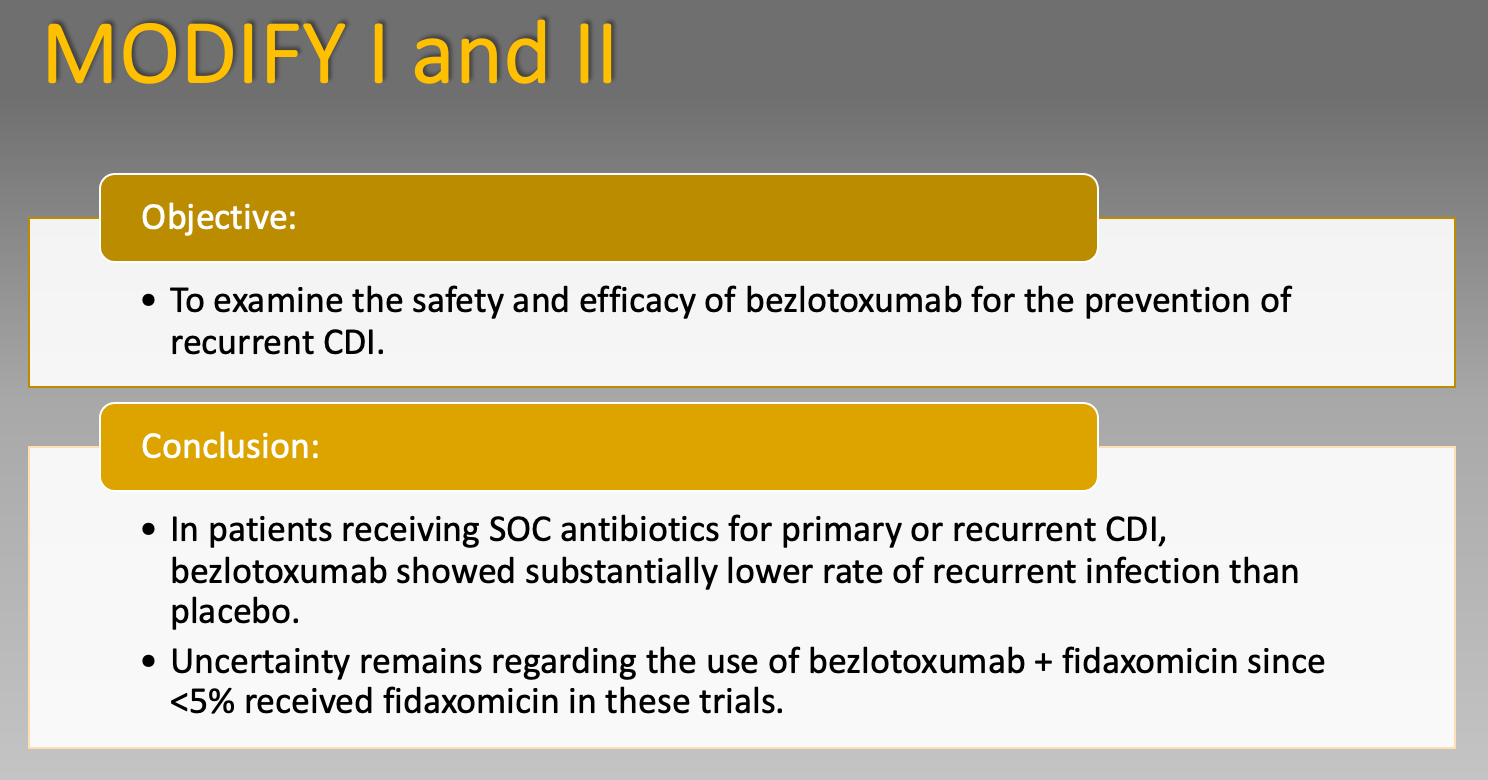
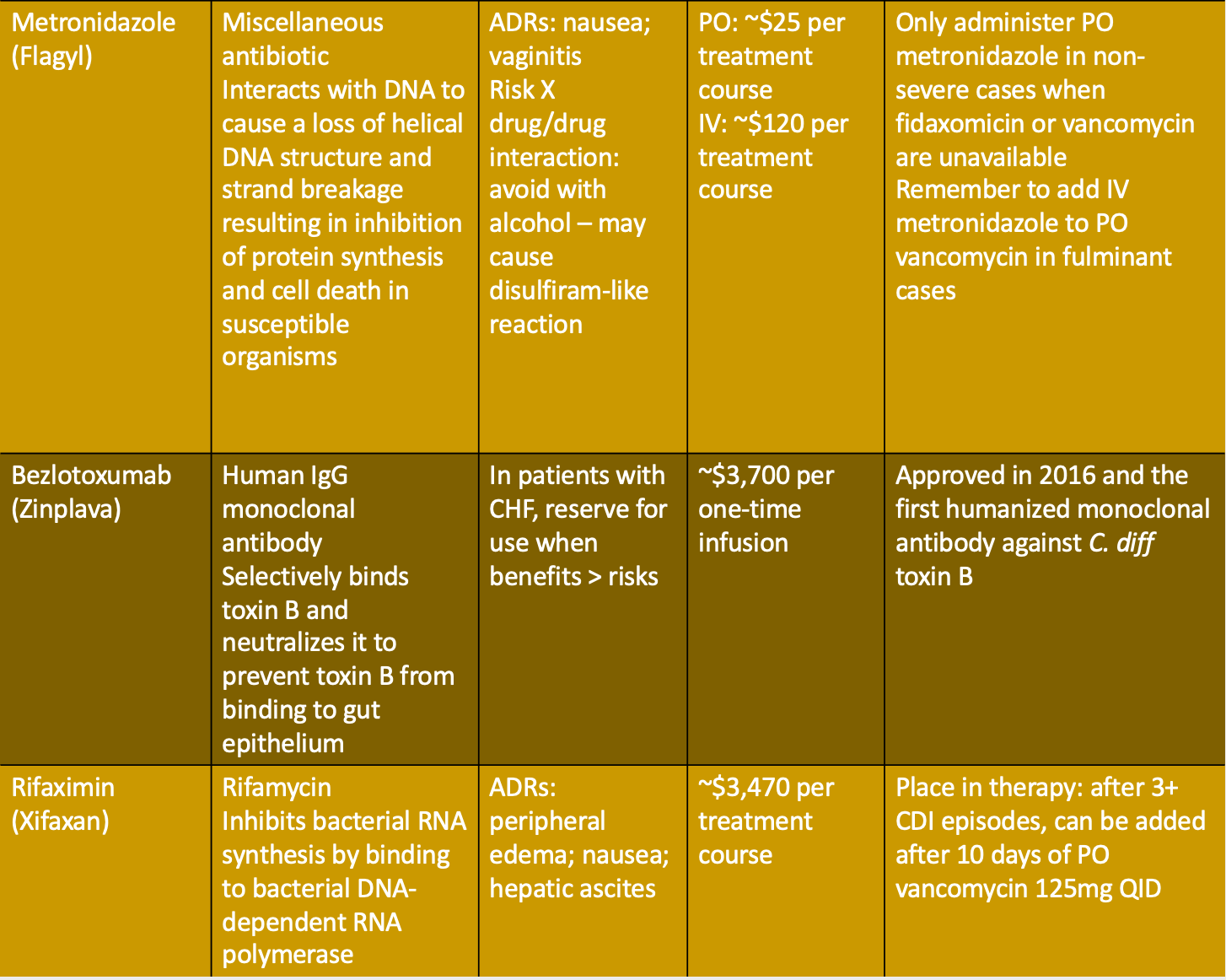
Update/question #3: In patients with a CDI episode, should bezlotoxumab be used as a co-intervention along with standard-of-care antibiotics rather than standard-of-care alone?
- Answer: Yes, updated guidelines suggest co-administration of bezlotoxumab along with standard-of-care antibiotics for patients with a recurrent CDI episode within the last 6 months.
- Evidence: Pooled analysis of 2 phase III clinical studies (MODIFY I/II).
Additional Treatment Notes
1. The offending agent that may have caused the CDI should be DISCONTINUED, if possible.
2. Electrolyte imbalances should be corrected immediately.
3. Fecal microbiota transplantation (FMT) = recommendations have not been changed for this (2+ recurrences of C. diff who have failed appropriate antibiotic treatments and where appropriate screening of donor and donor fecal specimens have been performed), but FDA outlines 3 separate safety alerts since 2019:
- Two alerts document transmission of pathogenic E. coli from donor to FMT recipient, some of whom became ill and some of whom died.
- One other alert is the concern for potential for transmission of severe acute respiratory syndrome coronavirus (SARS – CoV-2).
4. The role of probiotics: currently not recommended to administer probiotics for primary prevention of CDI – insufficient data to support the use and can potentially cause infections in hospitalized patients.

Medications
Conclusion/Pharmacist Pearls
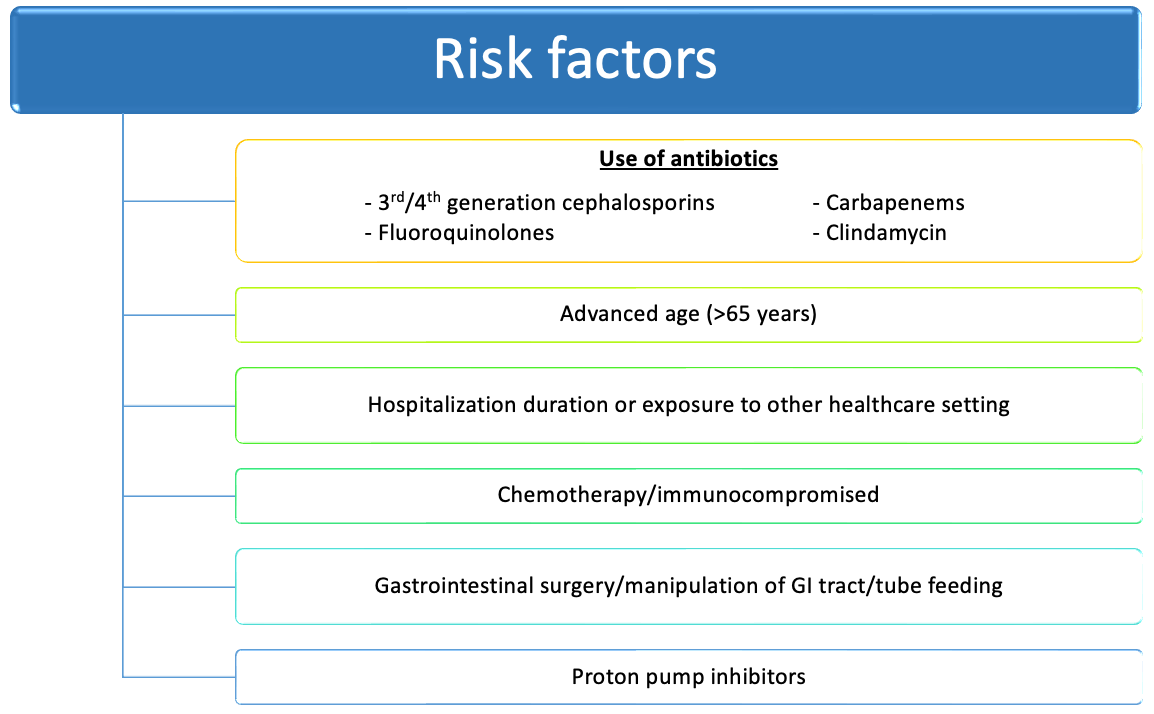
Remember the risk factors: Older age (>65) and use of antibiotics increases the risk of CDI.
If possible, discontinue offending antibiotic and correct electrolyte imbalances ASAP.
Discontinue unnecessary proton pump inhibitors (PPIs) – although a true causal relationship is unclear, several studies have shown that exposure to PPIs can increase the risk of developing CDI.
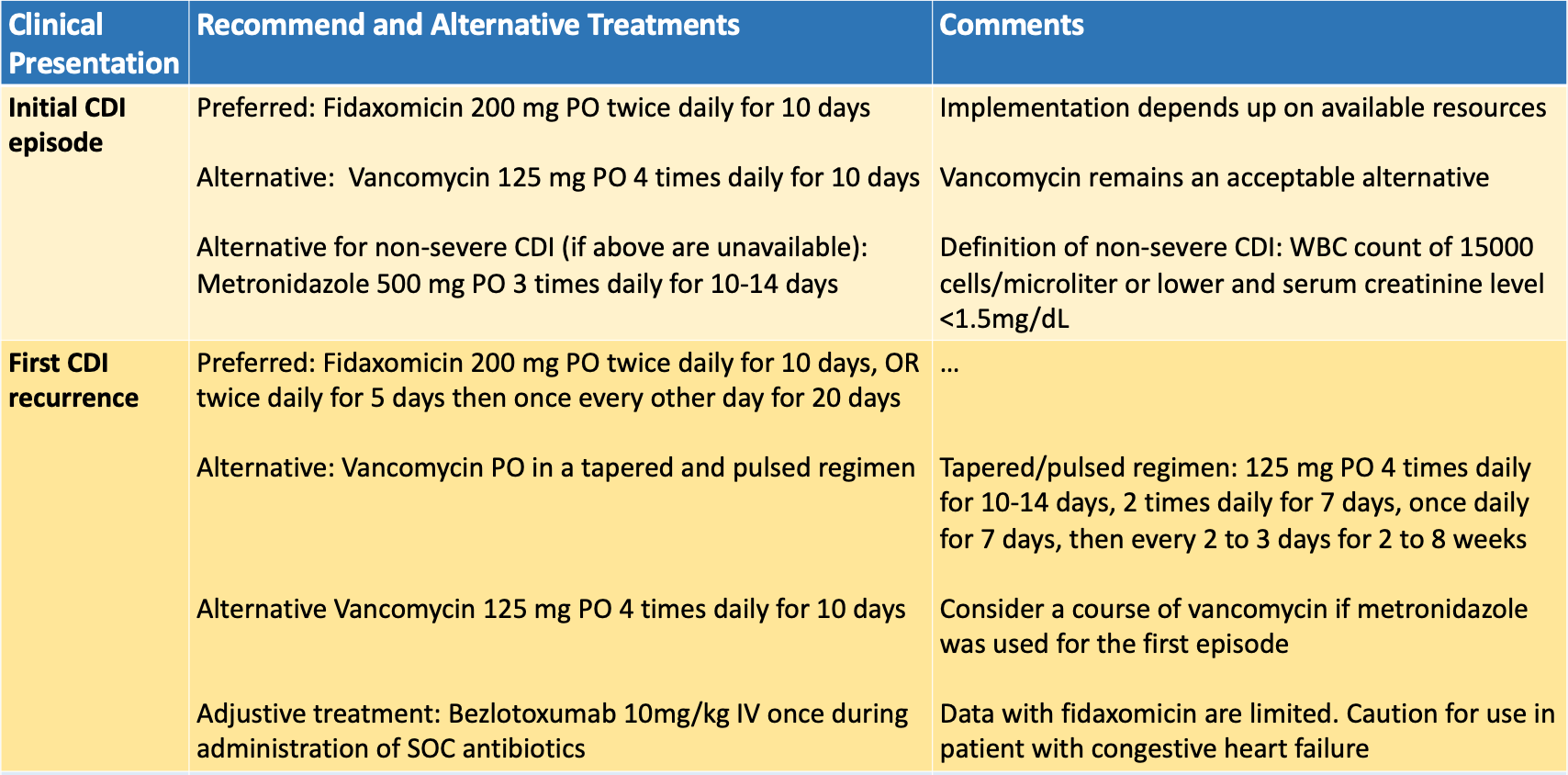
Initial CDI episode? Fidaxomicin preferred over oral vancomycin as RCTs showed sustained clinical cure.
Recurrent CDI episode? Fidaxomicin preferred.
High risk of recurrence? (ie, recurrent CDI episode within the last 6 months; age >65; immunocompromised host; or severe CDI on presentation): Adding bezlotoxumab to oral vancomycin therapy is encouraged.
Fidaxomicin: which dosing regimen – standard or extended-pulsed?
- Currently no comparative data of fidaxomicin standard course vs. extended-pulsed.
- Prior 2 studies in the 2017 guidelines used standard course, but the EXTEND trial studied the extended-pulse regimen due to in vitro human gut model study (showing persistence of fidaxomicin at the above inhibitory concentration which might prolong suppression).
- The EXTEND trial showed improved sustained responses and one of the lowest rates of recurrence ever reported, so I would recommend the extended-pulsed regimen if asked by a physician.
Patient Cases!
Patient Case, Part 1: PO is a 74-year-old male with PMH of COPD, GERD, T2DM, CHF, and HTN who presents to hospital with 5 loose stools within the past 24 hours. WBC 16,000; SCr 1.4; BP 141/91. Patient stated he was recently hospitalized due to a pseudomonal infection, but was then treated outpatient with an oral antibiotic. What possible risk factors could PO have for developing a CDI?
Patient Case, Part 2: PO ended up testing (+) for a CDI and was treated with Dificid 200 mg PO BID x10 days. Although Dificid has great data for preventing recurrent CDI, PO presents 1 month later with his first recurrent CDI episode. WBC 12,000; SCr 1.6; BP 147/93. Per current guidelines, what is the BEST recommended treatment of choice?
- A. Vancomycin 125mg PO QID x10 days + bezlotoxumab 10 mg/kg infusion
- B. Vancomycin PO in a tapered and pulsed regimen
- C. Fidaxomicin 200mg BID x5 days followed by once every other day x20 days + bezlotoxumab 10 mg/kg infusion
- D. Fidaxomicin 200mg BID x5 days followed by once every other day x20 days
(See comment section for answers)
Author bio: Ashley Wensing graduated with her Doctor of Pharmacy degree from Southern Illinois University Edwardsville (SIUe) in May 2022. She currently is a PGY-1 Pharmacy Resident at OSF Saint Francis Medical Center in Peoria, IL with interests in critical care and infectious diseases. In her free time, Ashley enjoys working out, playing piano, and traveling with her fiancé!

References
- McDonald C. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the IDSA-SHEA. Idsociety.org. Published February 15, 2018. https://www.idsociety.org/practice-guideline/clostridium-difficile
- CDC. C. diff (Clostridioides difficile). Centers for Disease Control and Prevention. Published July 12, 2021. https://www.cdc.gov/cdiff/index.html
- Carter GP, Rood JI, Lyras D. The role of toxin A and toxin B in Clostridium difficile-associated disease. Gut Microbes. 2010;1(1):58-64.
- Kelly CR, Fischer M, Allegretti JR, et al. ACG Clinical Guidelines: Prevention, Diagnosis, and Treatment of Clostridioides difficile Infections. American Journal of Gastroenterology. 2021;116(6):1124-1147.
- Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clinical Infectious Diseases. 2021;73(5):e1029-e1044.
- Guery B, Menichetti F, Anttila V-J, et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. The Lancet Infectious Diseases. 2018;18(3):296-307.
- Mikamo H, Tateda K, Yanagihara K, et al. Efficacy and safety of fidaxomicin for the treatment of Clostridioides (Clostridium) difficile infection in a randomized, double-blind, comparative Phase III study in Japan. Journal of Infection and Chemotherapy. 2018;24(9):744-752.
- Wilcox MH, Gerding DN, Poxton IR, et al; MODIFY I and MODIFY II Investigators. Bezlotoxumab for prevention of recurrent Clostridium difficile infection. N Engl J Med 2017; 376:305–17.
- Lexicomp. Siue.edu. Published 2022. http://online.lexi.com.libproxy.siue.edu
- Trifan A, Stanciu C, Girleanu I, et al. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World Journal of Gastroenterology 2017.