
Finding Nemolizumab in Prurigo Nodularis
Nemolizumab, when administered every 4 weeks, saw a statistically significant improvement in itch relief and IGA treatment success at Week 16, with results as early as 4 weeks, sustained/improvement through Week 24, and a relatively favorable safety profile.

Prurigo nodularis (PN) is a chronic, debilitating, neuroimmunologic skin disorder characterized by firm, flesh-to-pink colored, pruritic papules, plaques, and nodules.1 In fact, the word “prurigo” is derived from the Latin word pruire, which means itching, and “nodularis” is Latin for nodulus, or small knot. Nodules are small, raised bumps under the skin that can form in various parts of the body. However, in prurigo nodularis, they are typically distributed symmetrically on extensor surfaces of extremities and range from 1-3cm in size.
Prevalence
In the United States (US), the prevalence ranges from 37-148/100,000 adults and 7-22/100,000 children.2 Most patients are diagnosed from the ages of 40-69 years, with a mean age of ~51 years old, but it may occur in any age group. In fact, individuals with an atopic predisposition may have an earlier age of onset. It typically affects more females than males, and African Americans are 3-4x more likely to develop PN vs. white patients. Internal malignancy, renal failure, and psychiatric conditions may induce PN, and in HIV + patients, PN may be predictive of advanced immunosuppression.

Economic & Societal Burden
A 2023 review article on the burden of PN published in the American Journal of Managed Care reported the following statistics regarding PN’s burden within the US:3
- Societal lifetime burden: $38.8 billion
- Individual lifetime burden: $323,292
- Physician visits: 6.3 (SD, 3.3)
- Inpatient admissions PN vs. general population: 67% vs. 13% (p<0.001)
- Total ED costs: $4,377,553 (SD, $740,743)
- Average ED cost: $3,206 (SD, 397)
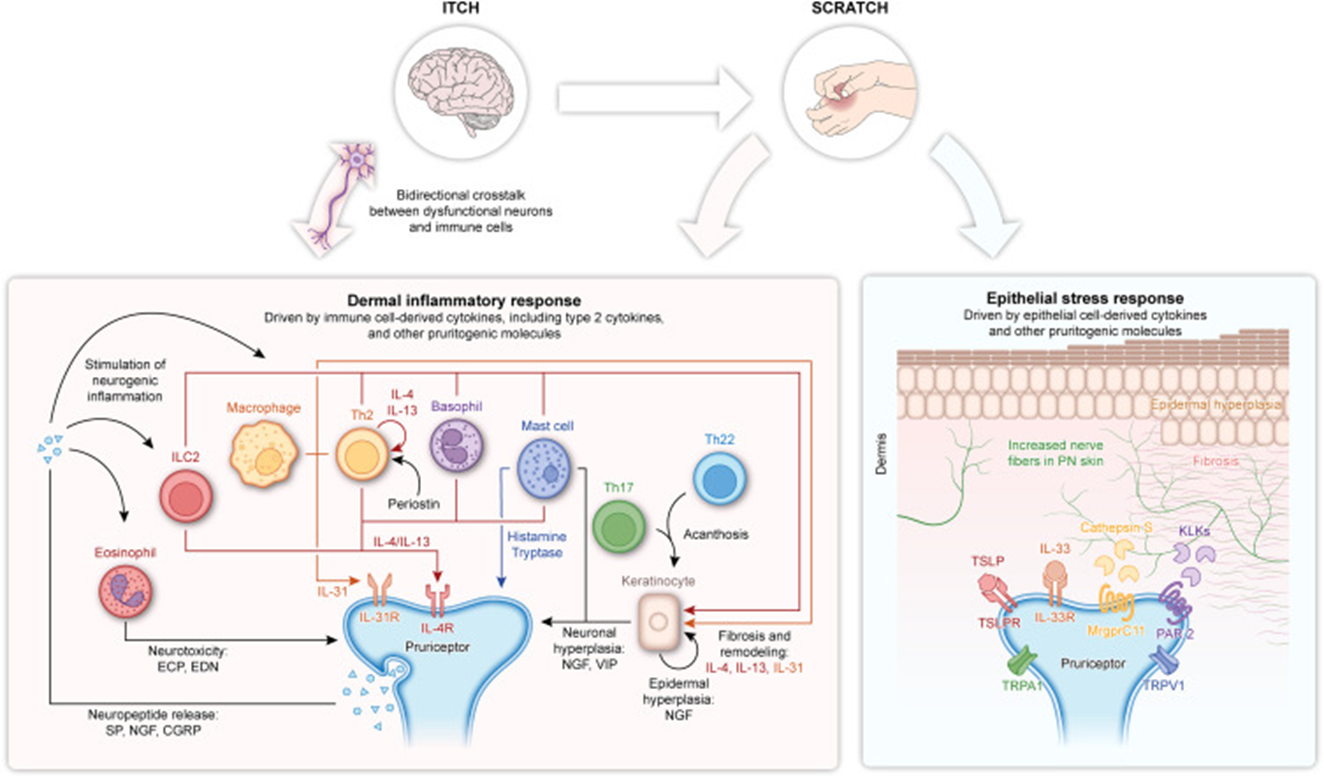
Pathophysiology
Prurigo nodularis involves skin lesions that result from chronic scratching driven by neuroimmunologic dysregulation.4 The pathophysiology is quite complex, involving Type 2, 17, and 22 immunologic pathways and the recruitment/secretion of T-lymphocytes, mast cells, and eosinophilic granulocytes. This generally leads to the inevitable itch-scratch cycle, a positive feedback loop where chronic scratching triggers additional pro-inflammatory cytokine release, which causes the patient to continue scratching.
Diagnosis
Patients must first present with a history of chronic, severe pruritis with excoriations and flesh-colored, pink, nodular lesions on extensor surfaces.1 A provider will typically perform a dermoscopy to rule out hyperkeratosis lenticularis perstans. A skin biopsy can also be performed for bleeding lesions, ulcers, or those resistant to first-line therapies. Underlying causes, such as renal, liver, thyroid disorders, HIV, malignancy, and/or parasitic infections, must be ruled out. For labs and tests, a provider may order a complete blood count and metabolic panel, thyroid stimulating hormone test, free T4, urinalysis, stool exam, HIV antibody, chest x-ray, and IgE level.
Management
The three main goals of care are itch relief, lesion healing, reduction of sleep disturbance, and quality of life improvement. Basic management involves:
- Short nails, protective clothing, and cover with bandages
- Bathe with gentle cleansers and apply emollients
- Calamine lotions + menthol/camphor for itch relief
- Cool, comfortable environment
- Reduce stress
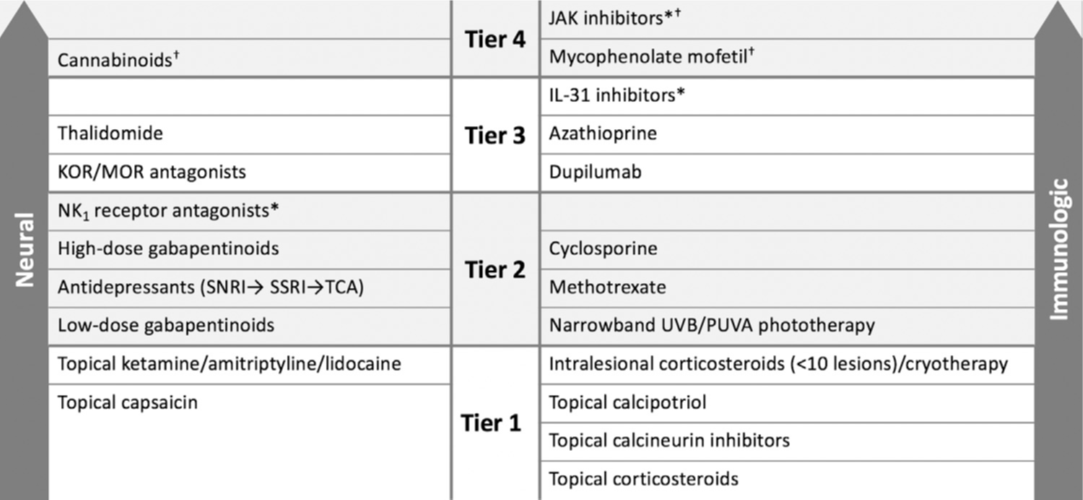
There are no formal US guidelines for the treatment of PN. However, a 2021 US expert panel involves the following panel, based on tiers.5 A holistic approach is recommended, targeting both neural and immunologic pathways, starting with more localized/topical therapies and transitioning to systemics/biologics in more serious/resistant therapies. Dupilumab serves as the first FDA-approved biologic as an IL-4 receptor alpha blocker, inhibiting IL-4 & IL-13 signaling pathways, from the pivotal LIBERTY-PN PRIME trials.6 58.8% of dupilumab vs. 19% of placebo patients saw a 4-point improvement in worst-itch numerical rating scale (p<0.0001), which is an 11-point scale from 0-10 that evaluates a patient’s worst itch over the previous 24-hours. However, there remains a great unmet need for patients not finding adequate relief, potentially involving a different, unique mechanism.
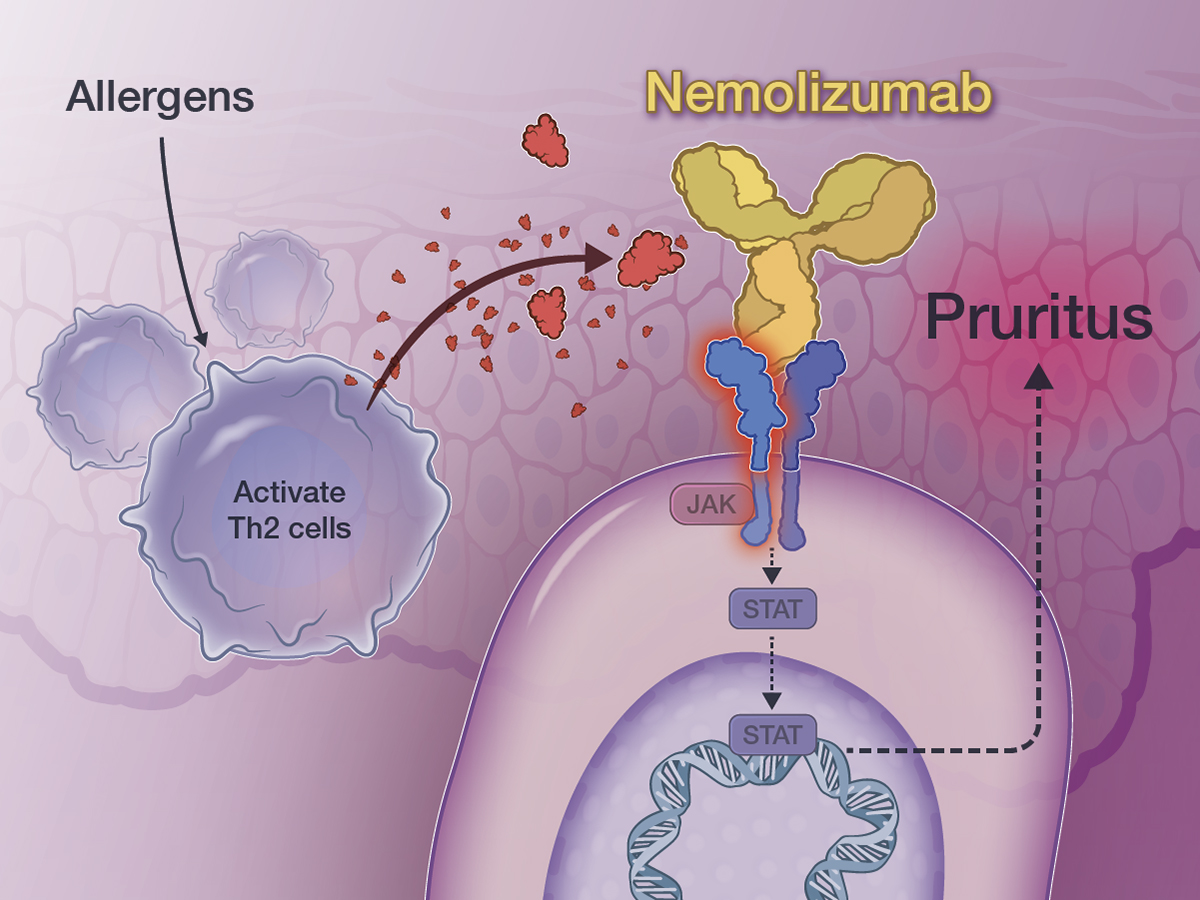
Nemolizumab
Nemolizumab (Nemluvio) was approved by the FDA on August 13, 2024 for the treatment of prurigo nodularis based on the pivotal OLYMPIA 1 & 2 phase 3 trials.7 Nemolizumab is a humanized IgG2 monoclonal antibody inhibiting the IL-31 receptor alpha subunit. It is administered underneath the skin, and presents with hypersensitivity and live vaccinations warnings and precautions.
The OLYMPIA trials were double-blind, multicenter, randomized phase 3 trials that randomized patients 2:1 to nemolizumab vs. placebo for 16 weeks (24 weeks for OLYMPIA 1) at 68 sites across 9 countries from 8/2020-2/2023.8 Patients received a 60mg loading dose following by 30mg (<90kg) or 60mg (>90kg) every 4 weeks. No topical calcineurin inhibitors, topical corticosteroids, oral antihistamines, systemic immunomodulators, nor “anti-itch” emollients were allowed during treatment. Rescue therapy was allowed at the investigator’s discretion (OLYMPIA 2), but patients were considered to have failed treatment. It was estimated that 270 patients were required for 90% power to detect a 2-sided 5% significance.
Inclusion criteria involved adults (>18 years old) with history of PN >6 months, investigator’s global assessment (IGA) of >3, severe pruritus (peak-pruritis numeric rating scale (PP-NRS) >7), >20 nodular bilateral lesions, and females of childbearing age using >1 method of contraception through 12 weeks after the last injection.
The co-primary endpoints were itch response (>4-point reduction in PP-NRS) and IGA response (0 or 1 with a >2-point reduction). Baseline characteristics were similar across groups, with ~60% females, mean age of ~53 years old, ~80% white, and ~78% receiving prior topical corticosteroids. Additionally, ~57% of patients had moderate PN, and ~37% had >100 nodules.
~57% of nemolizumab patients vs. ~18% of placebo patients met the primary endpoint of >4-point improvement in PP-NRS at Week 16 (p<0.0001 and p<0.001). Additionally, ~31% of nemolizumab patients vs. ~9% placebo patients met the other primary endpoint of IGA Success at Week 16 (p=0.0001 and p<0.001).
Regarding safety, the two most common treatment-emergent adverse events (TEAEs) were atopic dermatitis (~5%) and headache (~7%) . Overall, there were low rates of serious adverse events and those of special interest (injection-related reactions, new/worsening asthma, infections, peripheral/facial edema, and ALT/AST + bilirubin elevation.
Conclusion
Nemolizumab, when administered every 4 weeks, saw a statistically significant improvement in itch relief and IGA treatment success at Week 16, with results as early as 4 weeks, sustained/improvement through Week 24, and a relatively favorable safety profile. These results led to its FDA approval in PN as a new treatment option targeting a specific cytokine involved in the itch pathway. However, there still remains an unmet need for this complex neuroimmunological disease, with many pharmaceutical companies researching novel therapies.
References
- Mullins TB, Sharma P, Riley CA, Sidharth Sonthalia. Prurigo Nodularis. Nih.gov. Published September 14, 2021. https://www.ncbi.nlm.nih.gov/books/NBK459204/.
- Huang AH, Williams KA, Kwatra SG. Prurigo nodularis: Epidemiology and clinical features. J Am Acad Dermatol. 2020;83(6):1559-1565. doi:10.1016/j.jaad.2020.04.183.
- Chisolm SS. A Review of the Current Management and Burden of Prurigo Nodularis in the United States. AJMC. Published May 5, 2023. https://www.ajmc.com/view/a-review-of-the-current-management-and-burden-of-prurigo-nodularis-in-the-united-states
- Kwatra SG, Ständer S, Yosipovitch G, Kim BS, Levit NA, O’Malley JT. Pathophysiology of Prurigo Nodularis: Neuroimmune Dysregulation and the Role of Type 2 Inflammation. Journal of Investigative Dermatology. Published online August 30, 2024. doi:https://doi.org/10.1016/j.jid.2024.06.1276.
- Elmariah S, Kim B, Berger T, et al. Practical approaches for diagnosis and management of prurigo nodularis: United States expert panel consensus. J Am Acad Dermatol. 2021;84(3):747-760. doi:10.1016/j.jaad.2020.07.025
- Yosipovitch G, Kim BS, Kwatra SG, et al. Dupilumab improves pruritus and skin lesions in patients with prurigo nodularis: Pooled results from 2 phase 3 trials (LIBERTY-PN PRIME and PRIME2). JAAD International. 2024;16:163-174. doi:https://doi.org/10.1016/j.jdin.2024.03.025.
- HIGHLIGHTS of PRESCRIBING INFORMATION. Accessed November 3, 2024. https://www.galderma.com/us/sites/default/files/2024-08/Nemluvio_PI_USA_08_2024.pdf.
- Kwatra SG, Yosipovitch G, Legat FJ, et al. Phase 3 Trial of Nemolizumab in Patients with Prurigo Nodularis. N Engl J Med. 2023;389(17):1579-1589. doi:10.1056/NEJMoa2301333.
*Information presented on RxTeach does not represent the opinion of any specific company, organization, or team other than the authors themselves. No patient-provider relationship is created.